Executive summary
This is the evaluation report of the 2012 'Social Assets in Action Project', led by IRISS, East Dunbartonshire CHP and East Dunbartonshire Council, with support from the Third Sector.
The report may be of particular interest to those concerned with a focus on strengths in professional practice as distinct from promoting a focus on assets in community development.
The Project aimed to incorporate strength-based practice in the delivery of mental health services by piloting Personal Asset Mapping, and to broaden awareness of community assets in order to show options outside of public service delivery including through developing a Community Well-being (asset) Map. This was intended to complement rather than replace attention to the needs of people who use services.
Personal Asset Mapping (PAM) is the practice of making a visual representation of the positive influences in a person's life.Personal Asset Mapping, with its visual approach, can make a big difference to people who use services who try it. This can occur after even just one session making a map and so has great potential to promote well-being. As one person who uses services said:
It's a like a grateful list on a bad day when you feel there is nothing to live for - writing stuff down makes you aware of what you have. I didn't realise what I had. It makes me think about why I do some things and how I could make more use of things that are on the outskirts. It made me widen my interest areas.
The project measured mental well-being of people who tried PAM, before and after they tried it. The results indicate that trying PAM may increase mental well-being slightly and that being supported by a practitioner to use a PAM may increase mental well-being significantly, however further research is required to confirm or reject this. PAM does not have negative effects in and of itself but, because it can prompt reflection and comparison, a therapeutic relationship with a practitioner can make a difference to how productively it is used.
Personal Asset Mapping allowed most practitioners to put their person-centred and recovery-focused intentions into practice, however good use of PAM requires a facilitative approach, which Practitioners based in the public sector found harder than those in the third sector.This finding has wider implications for development of new practice- system and individual capacity for adaptive practice is an underpinning requirement.
The Community Well-being Map, documenting the assets mapped by the project, is live at http://www.eastdunassets.org.uk/ and has initially been well received.If promoted and used well, in the longer term it may lead to an improvement in people's views of East Dunbartonshire as well as leading to more action by community members to promote their own well-being.
- The project also makes a contribution to learning about personal and community asset mapping in practice:
- Allow control for people over sharing the meaning of their PAM with others.
- Create PAMs as a support planning tool and use to reflect on progress.
- A choice of paper or digital PAM should be offered to everyone using services.
- Refer to and update the model of practice developed by this project when further testing PAM
- Asset Mapping Workshops generate qualitative data that make the Community Well-being Map (CWM) engaging and drop-ins generate volume of assets.
- Support people who already have good knowledge of a community- Connectors- to spread awareness and use of the CWM, rather than only relying on organisations, ensuring the needs of those who don't use the Internet are considered.
The Project Partners should now develop a whole systems approach to focus on assets; building on the tools developed in this project e.g. by deciding how assets-focus can be supported by performance measurements, how the CWM can be drawn on in Community Planning, and what changes to infrastructure are needed to maintain momentum.
Background on assets
An emphasis on strengths
Asset-based approaches aim to identify the resources, strengths and capabilities that exist across communities, groups or individuals through engaging with community members (Lynch, 2010). They are often presented as a challenge to 'deficit' approaches, which emphasise problems and needs, and are held to be:
- More widely practiced, dominant and/or traditional (Graybeal, 2001, Pattoni, 2012a, Burns, 2011)
- Damaging because they emphasise problems (Kretzman and McKnight, 1993) and
- Damaging because they stigmatise groups (Cook and Khotari, 2001, Lynch and Allan, 2008, Bogenschneider and Olson, 1998)
Core concepts
In Scotland the Chief Medical Officer, Sir Harry Burns, included a chapter on Assets in his Annual Review (Burns, 2011), introducing the theory of salutogensis. Antonovsky, who established the theory of salutogensis to promote focus on causes of good health and not just focus on causes of illness (i.e. pathogenesis), set out two main salutogenic concepts (Antonovsky, 1979). These are firstly generalised resistance resources; factors such as social support, knowledge, money, self-esteem, which may be thought of as assets, and secondly a sense of coherence including comprehensibility, manageability and meaningfulness, which may be thought of as the capacity to deal with whatever happens in life by drawing on assets.
Assets focus- challenges and opportunities
Asset mapping is a visual approach to documenting a range of strengths. Some critique of the asset-based discourse exists, on the basis that it may distract from addressing income inequality, which some think may be more significant to health than focus on deficits (Roy et al, 2012). However Friedli (2011) suggests that 'Comprehensive asset mapping could provide a framework for asking new questions about equitable access to valued resource', and that ownership of resources should also be questioned.
About the project
IRISS (Institute for Research and Innovation in Social Services), East Dunbartonshire Community Health Partnership (CHP) and East Dunbartonshire Council (EDC) were lead partners in the Social Assets in Action pilot project from May to December 2012. Many other organisations also leant their support, including EDAMH, EDVA, The Richmond Fellowship and Carers' Link. It was part funded by Better Together, a Scottish Government patient experience improvement fund. This pilot followed on from a proof of concept project run by the same partners in 2011, focused on Kirkintilloch.
Objectives
This project aimed to broaden the approach to intervention for health, to increase attention to assets, rather than to ignore or diminish need.
Specific objectives included:
- To shift the role of service provision to focus on a strengths-based model.
- To encourage individuals' self-efficacy in respect of accessing and using assets.
- To improve patient experience of accessing support in the community through practitioners focusing on strengths and identifying personalised options.
The project addressed these objectives by embedding Personal Asset Mapping (PAM) practice within mental health practitioners' support to individuals; thereby increasing focus on resistance resources and promoting sense of coherence through practitioners' therapeutic support to individuals.
Further objectives were:
- To create resources for practitioners and individuals to embed the approach in service provision by developing a digital tool.
- To encourage choice in service provision; building community knowledge on assets through creating a community asset map website that may be used by individuals and professionals.
To achieve these objectives an iPad app version of the Personal Asset Map and a website detailing community assets have been developed. Knowledge of community assets was generated via a series of workshops and drop-ins held in all the towns in East Dunbartonshire.
Outcomes of Personal Asset Mapping
This section of the report answers two key questions:
- What difference did the Personal Asset Mapping approach make to people who use mental health services?
- What difference did Personal Asset Mapping make to mental health practitioners' professional practice?
Personal Asset Mapping and people who use services
Personal Asset Mapping has great potential to effect a positive change in the extent to which people take action for their own well-being and consequently to improve their mental well-being. The act of making a map also supports a small short-term improvement in mental well-being.
Personal Asset Mapping was very powerful for some people; as a person who uses mental health services explained their experience of having recently tried PAM
'It gives me perspective. My family deserves more attention that I have been giving them. I feel it is time to take control and so I've been calm all week. I've been able to sleep and am taking control because I've re-prioritised.'
The evaluation captured feedback from 21 instances of people developing a Personal Asset Map in a one-to-one context, i.e. in the course of support provided by a mental health practitioner. Feedback was also collected from a further 18 people who tried Personal Asset Mapping in a peer-support group.
Personal Asset Mapping made a difference to people by:
- Making them more conscious of the positive things and people they have in their lives. This appears to occur for everyone and to have a small positive effect on mental well-being.
In some cases this led to the Personal Asset Mapping process:
- Helping them to set goals for improved use of assets. Some people appeared to do this spontaneously, others with support of a practitioner and some did not appear to have been supported to do this.
Where this did happen it led to the Personal Asset Map:
- Supporting improved use of assets. This happened as a function of the PAM being a personal visual reminder of goals and/or as a tool to support facilitation by practitioner. This did not occur for everyone within the timescale within which results were being observed.
This meant:
- Some people started to change relationships, try new things (community activities), or make more use of existing assets. This appears to have had a large positive effect on well-being.
Each of these changes is discussed in the following section, which then also includes a discussion of the evidence for initial and longer-term changes in well-being.
Raising awareness of assets
Feedback from individuals who tried Personal Asset Mapping suggests that it encouraged individuals to look more positively at their lives, which lead to them feeling better about themselves and their lives. They reported
'It made me realise I had lots of friends and opportunities to develop'
and
'Surprised how much I could put down and much was important to me. Felt quite good doing it'
and
'Realised how much my Dad is important in my life.'
Practitioners reinforced this point in their perception of how people found it
'She surprised herself by how she was reacting to mapping'
. Some people had realisations that made them upset but this did not last. Another practitioner reported how making the map had been important to trying to focus on the positives
'One of the people I support has a personality disorder and turns every positive into a negative. The map gave some concrete evidence that actually he had a lot of good things going on. He couldn't argue with it'
An initial theory of change developed with project staff prior to the project commencing anticipated that well-being would only improve after some action had been taken to change use of the assets that had been mapped. However well-being did appear to increase immediately, this is discussed further under the 'increased well-being' heading below. Seligman and colleagues (2005) suggest this effect is to be expected.
Visuals prompting action
Some of those who developed asset maps found that it led them to set goals or attempt to take action without prompting from a practitioner. Reports highlight the importance of the visual aspect of mapping to this; e.g. a person who uses services said
'It made me see the big picture'
and another said
'I feel I've moved on quite a bit. I could see what I have to work on next. Getting back to my hobbies which I have problems with at the moment due to health problems'
and another '
it wasn't anything that I didn't know but I have been thinking about it. I was thinking about whether or not I should move things around'
(emphasis added).
In other cases the asset map did not appear to prompt self-motivated action but did open up new therapeutic opportunities by improving communication with the practitioner about what was important to the individual. Again visual aspects were highlighted as important, with practitioners reporting that what worked was
'Working together, having visual aids'
that it
'helped people see or just think about what were the assets in their lives'
and that '
It lets you see a relatively clear picture of what you have or don't have in your life, makes you think can give a clear message to a practitioner of where someone is with their life'
(emphasis added).
This enabled increased focus by the practitioner on helping people to make goals and tackle problems in making sense of, and drawing on, a range of well-being-promoting factors. Practitioners reported things like
'(I valued) the discussions that came up as a result of where things were being placed on the map'
and
'I discussed things with service users that I may not have if we hadn't went over asset mapping.'
and '
During the asset mapping I discovered that he was feeling frustrated with his artwork. He finds it so important that it overwhelms him.'
There is evidence from others that indicates visual methods can help to improve support; e.g. Griffiths and colleagues (2007) and Czuchry, Newbern-McFarland and Dansereau (2009). There is also evidence that this is in part achieved by opening up new conversations; e.g. see the Talking Mats approach that is used for people with dementia (Murphy, Gray and Cox, 2007), use in social research (Banks, 2001) and use in service design (Brown, 2008).
There was a small group for whom asset mapping did not seem to prompt any specific thoughts about changes from them and whose practitioner did not seem to have encouraged it. One person resolved that they were happy with how things are '
There was nothing that surprised me too much; it just showed me that I have a pretty full week of things.'
Others may yet find themselves prompted to reconsider their asset map with support later.
Taking action
Even in the short timescale of the week between doing an asset map in the group session, and the subsequent week when the experience was discussed, some people made changes as result of having done an asset map, e.g.:
I have a problem with a group of people. I have tried to be helpful to people but it backfired. In the last week I looked at the things on the map differently. Afterwards I had stomach cramp but it was good for me to look at who is important in my life and I see I needed to shift the people who weren't doing me any good to the outer limit. For the first time in my life I am clear that I feel I have done nothing wrong. (Person who uses services)
Some of those who were supported one-to-one also started to make changes immediately, e.g.:
I've been letting more people into my life. Concentrating on it and seeing he names that I've written on it helps me to bring people in. With other types of support it's just chatting but with this we can see it and we can talk about I might move people. I joined a volunteering group as well (Person who uses services)
I discovered that he has a Dad who he never sees; this is an underlying problem for him. Has many online friends but hardly any he would meet up with. This all brought up conversations which I hadn't had with him before, leading me to provide him with new self help materials. (Practitioner)
One of the two I did it with was quite good and there was a change. He didn't have so much in his life because he's lost two people in the last year. So we looked at what could go into the gaps. He started an adult education class. He used the initial map to build on so he could add things in. (Practitioner)
This positive feedback supports that people do use their map to plan and to take more positive steps and can be supported to do so, how long changes last, and what else happens, still remain to be tracked.
Increased well-being
There are indications that Personal Asset Mapping increases mental well-being in two ways. Firstly it may increase well-being a little in the short term amongst most of those who try it. Secondly for those who chose to and are supported to make changes in their life, mental well-being may increase further.
Measuring well-being
The Warwick-Edinburgh Mental Well-Being Scale (WEMWBS) was used in order to provide an indication of the mental well-being of the people who use services before and after they tried asset mapping in a one-to-one setting. It comprises 14 items scored from 1 (none of the time) through to 5 (all of the time). Examples are: 'I've been feeling good about myself'; 'I've been feeling useful'. A shorter, 7 item version (SWEMWBS) was used with the people in the Connections peer-support group to minimise the time required for completion.
High scores represent greater mental well-being, with the minimum for WEMWBS being 14 and maximum 70, and half of this for SWEMWBS. Normative data from WEMWBS are available from Tennant et al (2007) based on 1,749 respondents to Scottish surveys in 2006. The National population median score was 51 with interquartile range of 45 to 56. The national population level distribution of SWEMWBS is not known, however it may be assumed to be similar to WEMWBS (Deacon et al, 2009), with scores of half of the full version of WEMWEBS, therefore we might expect a median score of 25.5 in the Scottish Population on SWEMWBS.
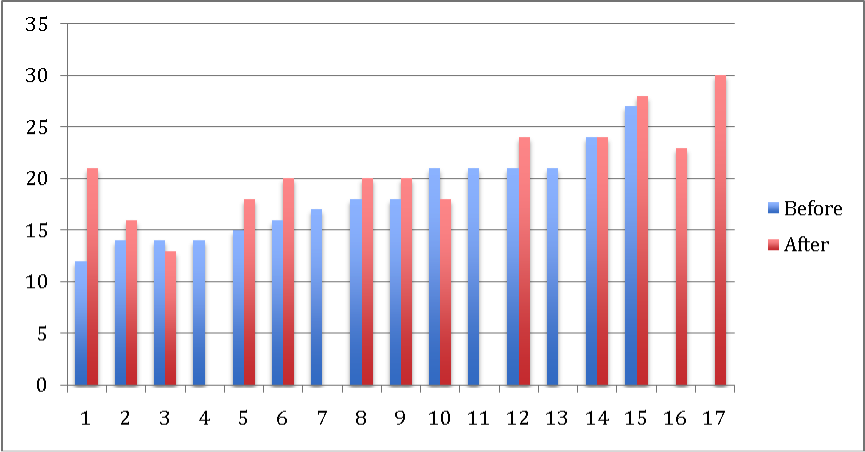
Results for those supported one-to-one
A WEMWBS score was calculated for 16 people prior to trying Personal Asset Mapping and 15 people after trying Asset Mapping (since one person did not complete a second WEMWBS survey). All 14 items were completed in all cases. WEMWBS surveys were filled in an average of 38 days apart. Practitioners were asked to request the second survey after they had started a PAM and then had a subsequent appointment at which they discussed or developed the PAM further. Figure 1 shows the before- and after- readings.
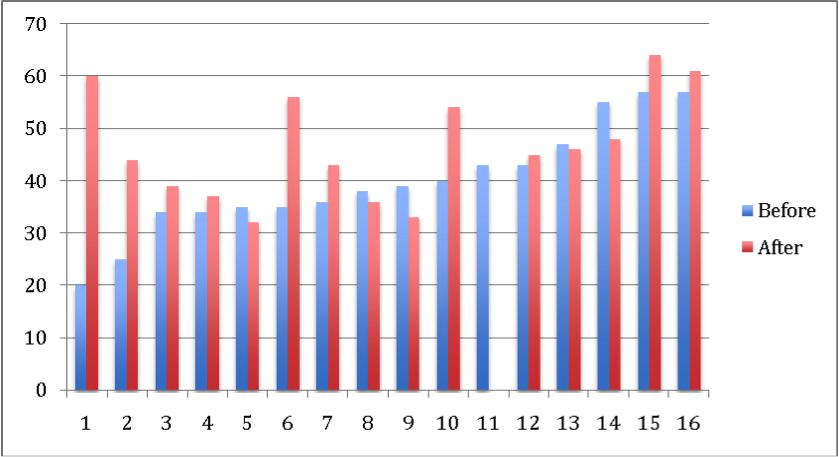
Most (10/16) people reported an improvement in well-being and the individual with the lowest initial well-being reported a very large improvement in well-being.
The median of the before (38.5) and after (44) scores are both significantly lower than the Scottish population norm (51). The scores before trying Personal Asset Mapping are even lower than those in the Scottish population with 'very poor' self-perceived health status, who have a median of 41 (Tennant et al, 2007). Whilst no normal population score for those in receipt of mental health services appears to be available, the low scores are probably not surprising. They may also indicate that practitioners did not (or could not) pick a group with higher initial well-being to try PAM with.
Conclusion
Personal Asset Mapping may have contributed to a large (mean 8.5 points) improvement in mental well-being in most (10/16) of the participants, and it may have contributed to, or at least not avoided, a smaller (mean minus three points) deterioration in mental well-being in the remainder (6/16) of participants.
There are two notes of caution; WEMWBS has not yet been validated for monitoring change in mental well-being in individuals and the small sample size achieved in the project limits confidence in the results.
However, in support of the results, narrative provided by practitioners was matched to half (8/16) of the cases, three whose score improved and five whose score declined. These can be used to support a view that the positive changes were mostly as a result of initial changes helped by starting a Personal Asset Map. For example, the story behind the person whose WEMWBS scores changed the most (from 20 points to 60 points) included 1) Discovery of both activities and people that were positive but that the individual had trouble drawing on 2) Motivation on the part of the individual to change the situation and 3) Assistance from the practitioner to support the individual to start to make changes. The negative changes in others appear to either be unrelated to PAM (3/5) or to relate to people whose initial assessment of their situation having started an asset map was negative (2/5). In these last two cases practitioners described a course of action that had been put in place that may lead to positive results later.
Well-being in those supported in a group
A SWEMWBS score was calculated for 15 people prior to trying Personal Asset Mapping in the first week that the project team visited the peer support group. A SWEMWBS score was calculated for 13 people who filled out the survey in the second week that the project team visited the group. 11 of these 13 were scores after one week from those who tried PAM in the first week and two represent scores of people who did not attend in the first week. All seven items were completed in all cases. The scores are shown in figure 2 below:
One individual, who started with very low well-being, reported much higher well-being in the second week. The others show a more modest increase, and in two cases a small decrease.
Observations
These scores suggest that the well-being of the group before trying PAM was lower than the well-being of the individuals supported in a one-to-one setting since the median (18) and interquartile range (14-21) are all less than half of the full WEMWBS scores.
The mean difference in before- and after- scores was two points; with insufficient data to calculate an interquartile range, meaning we cannot be very sure of the results. There were two outliers, one whose score changed by minus two and one whose score improved by nine points.
The well-being of the group after trying PAM was still less than half (median 20) of the after score in the group supported one-to-one.
Conclusion
Compared to the people who were supported one-to-one over a longer time frame, there are indications that one Personal Asset Mapping session in a group results in a smaller (but more even across the group) improvement in well-being. It is likely that, by supporting these people to make use of their maps over time, a greater increase in well-being would have been observed.
One benefit to the evaluation of having this group try PAM is that, given the second measurement was taken only one week after the intervention, the case for attributing the change in this group to the PAM exercise is relatively clear. This is in comparison to people supported one-to-one, whose outcomes may have been affected by other actions and circumstances in the weeks between appointments.
A larger sample of WEMWBS readings from people who try PAM, together with a comparison group, is required to confirm or reject this conclusion.
Effect of Personal Asset Mapping on practitioners' professional practice
As a result of the project practitioners became more confident about using the PAM approach and those in the third sector were the most enthusiastic adopters. The most significant impacts that Personal Asset Mapping had on professional practice were that it increased the extent to which professional practice exhibited person-centred and recovery-focused characteristics.
These changes occurred as a result of practitioners attending two workshops to try PAM, consider how it fitted into their practice, and plan their approach to trying it with three individuals they support (in practice most tried it with fewer than three people). They reported on their experience of introducing it to people as an option and of trying it in a diary, at a workshop and in phone interviews. The results are described in this section.
Being more person-centred in practice
Personal Asset Mapping helped practitioners to find out more about a person's life, even when there was a therapeutic relationship spanning several years. Personal Asset Mapping is therefore strongly supportive of person-centred practice, e.g. a practitioner said
'In the past you might not have dug deep enough about what people want because you're thinking about their health. Now you're thinking about a broader range of stuff.'
Practitioners said that they personalise their support, prior to trying PAM, but their answers about how they did this lacked depth. It is clear that more of the whole persons' life was explored in PAM and that this was different from previous practice; e.g. it was
'sometimes quite personal thing to do when a worker'
(referring to the nature of the topics explored). Therefore, there was a shift in the extent to which support was actually person-centred rather than simply intending to be.
Being more recovery-focused in practice
Personal Asset Mapping supports recovery-focused conversations.
Andresen, Caputi and Oades (2006) set out five aspects of engagement with Recovery, which they highlight are not sequential but are rather aspects that people can cycle between. These are shown in figure 3 in the left hand column. The opportunities for a focus on recovery using PAM, and the extent to which these were demonstrated in the project are mapped in the right hand column.
In short, PAM made practice more focused on:
- Raising awareness of positives; promoting hope
- Helping people to prepare
- Helping people to set goals and
- Helping people to self-manage by expanding the range of things that they do
| Aspects of Recovery | How PAM supports |
|---|---|
| Moratorium - a time of withdrawal characterised by a profound sense of loss and hopelessness; Awareness - геallsation that all is not lost and that a fulfilling life is possible. | It might be inappropriate to introduce asset mapping here, but having previously done an asset map might offer a way to engage with someone in Moratorium. Further research would be required. |
| Awareness - геallsation that all is not lost and that a fulfilling life is possible. | Having previously done a PAM might help people to gain awareness more quickly. Doing a PAM might help people to realise that it is possible to lead a fulfilling life. This was indicated to some extent by comments made about trying PAM. |
| Preparation - Taking stock of strengths and weaknesses regarding recovery and starting to work on developing recovery skills. | PAM is most obviously supportive of this aspect of recovery since it supports people to take stock of strengths. There were many examples of how PAM helped identify strengths and, although these did not tend to include personal strengths. This focus could be introduced in future. |
| Rebuilding - actively working towards a positive identity, setting meaningful goals and taking control of one's life. | There was some evidence that PAM prompted or supported people to set meaningful goals as highlighted in the earlier section of the report on outcomes for individuals. |
| Growth - living a meaningful life, characterised by self management of the illness, resilience and a positive sense of self. | Referring back to a previous PAM was thought to be positive in supporting a positive sense of self and self care. |
Potential impact of community asset mapping
A community asset map is now live at http://www.eastdunassets.org.uk/ This website (now called the Community Well-being Map; CWM) has potential to be of great use to the community, may promote a sense of pride in the community, and may also be used by professionals to help people find community assets, not just services. The website has been well received initially and judged to be informative and easy to use.
This section reports on the impact of the process of generating the map through community asset mapping workshops and early views on the potential impact of the map itself.
Outcomes of the community asset mapping workshops
The community asset mapping workshops improved people's opinion of the community, they learnt about assets and they intended to take more action to promote their well-being.
Opinions of the community
Most people attending the community asset mapping workshops reported that they thought more positively about their community at the end of the workshop, e.g.
'I'm surprised at how much there is to do'
and '
it changed my view of things round here'
. They said that there was more going on in their area than they had thought and this applied even to those people who were very active and connected locally e.g.
'I was very impressed with the session I went to (...) although I knew about most of the places (...) I did find out about a couple of places that I might go to (...) It make me think I was lucky to live here and surprised that there was more than I thought.'
Increased attention to assets
Most people (8/10 respondents) agreed or strongly agreed that they found out about assets they could use to promote their well-being at the workshops and all (10/10) agreed or strongly agreed that they would do more to promote their own well-being after the workshop. At five of the workshops people were offered coloured dots to mark the assets that identified what they planned to try. People were most keen to try social and outdoor assets but, conversely, assets categorised as 'skills and learning' were not frequently marked.
A response to the survey sent to workshop participants just after the Community Well-being Map website went live suggests that at some people may have followed up on their intention
'I went for a walk exploring with my son, helped us to communicate with each other on a neutral subject'.
This indicates that the community map may encourage people to try new social activities and be more active, which are both important aspects of promoting well-being.
Potential impact of the Community Well-being Map
Community and individual use of the map
Those who were shown the map seem interested in it saying e.g.
'Its very useful to have everything in a central reference point- there's a couple of things I've been told about that I've forgotten (so I can look there)'
and '
I'd use it to find out what people like to do; what's good is that people can comment'
and
'lets you know what is going on in the community and access the areas you want to go'
. Nearly everyone (10/11), feeding back after attending a community asset mapping workshop, said that they would use the map and the same number said that they would definitely or probably contribute to the asset map. Indeed 67 assets were contributed by text line by people who found out about the map at drop-ins, workshops or through others.
Other individuals who had been shown the asset map thought it was a useful reference e.g. some hinted that it might reduce isolation e.g.
'clicking on to something helps you feel less isolated and helps you think about what you might do.'
and that it can widen perspectives
'I looked outside of services and varied the places I went to.'
Of the four people that are known to have been introduced to the original Kirkintilloch map (as new maps had not yet been launched) by their practitioner, two appeared to find it useful. Practitioner comments on this were '
(...) it motivated them to attend fitness classes in local gym'
and '
one thought it was a great idea and spent the appointment looking through, trying to identify opportunities for himself.'
In the same way that PAM may have an initial impact on the well-being of people trying it, being exposed to the Community Well-being Map may have the effect of creating a more positive narrative and increased pride in East Dunbartonshire. As one person who uses services put it
'It challenges perceptions that there's nothing to do.'
Linking people to assets
Practitioners can be expected to use the CWM to link people to assets, since awareness of community assets amongst public sector practitioners was initially low (6/14 did not mention community resources, only services) yet they rated the importance of focusing on strengths highly, e.g.
'It's the crux of what I do. Incorporating changes in lifestyle to help emotional and physical well-being and always reducing the risk of relapse',
Third and public sector professionals attending a workshop to feedback on the CWM when it first went live though that would be helpful for:
- People new to an area
- People with dementia (good that its pictorial)
- People who don't qualify for social work support
- Staff to make it easier to answer enquiries about what's on.
These points could all be turned into opportunities to raise awareness of the map; e.g. by promoting it through estate agents, but to achieve real change people will need to use the map not just to know about it. Community Connectors attending the community asset mapping workshops saw its potential for community development e.g.
'it could be used to show people more ideas for what they could get involved with.
' so this group must not be overlooked in promoting it. If used well there is much potential for impact, e.g. it could
'Help people to spend leisure time close to home, helping the community to get to know each other, supporting the local economy and local jobs, maybe getting local people back to work or helping in their community'.
The Community Well-being Map has great potential but the strategy for its promotion must include encouraging people to use it, working with community members not just agencies, embedding in decision making such as Community Planning Partnerships, prioritisation of effort and reflection on what is working over time.
Learning from Personal Asset Mapping
This section presents some of the learning about the challenges of developing and spreading Personal Asset Mapping practice in order to promote well-being. There are five sections:
- How and when it can be used
- Negative and neutral effects
- Getting started
- Barriers to widespread use of PAM
- Barriers to using PAM to potential
How and when it can be used
The practice of making a paper-based PAM leaves the option to create visuals without necessarily documenting a detailed explanation of the meaning of the map to the person making it. This aspect of anonymity has been maintained in the development of the digital tool; labels and details can be added but don't have to be. This feature is important; e.g. in a group context people wanted to create a map the full meaning of which was apparent only to the individual creating it and felt that
'Having a password (on the digital version) would be good- might encourage me to be more open.'
In a one-to-one context it was the act of asking questions to establish meaning that opened up new conversations. Therefore it should not be a condition of starting a paper or digital map that the full meaning of a map is made transparent.
Practitioners with experience of trying the tool were asked how they thought it could be used in future. Answers included
- When someone is new to a service, particularly as an approach to broaden focus from any initial needs-focused service plans.
- At intervals to help someone to see their progress. This is supported by one of the Connections peer group members
'I have done asset mapping before about 6 months ago. It made me realise how I have moved on more than I realised. I think it is a good idea to review it every so often.'
- At points of transition and to aid decisions; e.g. when someone is about to leave a service or is planning ahead
'One of my clients is trying to decide which country she should live in so we are going to use mapping to give her a visual representation of what her life may look like'
- As a complement to other approaches,
'WRAP is quite good but its good in a group session. The size of the document can be a bit off putting. Everyone's different but asset mapping might be more flexible.'
Negative and neutral effects
Some people appear to gain more than others from Personal Asset Mapping but it is not easy to predict who would gain before it is tried. Not all of those who tried Personal Asset Mapping liked it or reported any benefit from it. It does not, however, appear to have had any negative effects; these were checked for.
Reports from practitioners about limited apparent impact included
'First individual engaged really well, there was no particular response that stood out, seemed open to try it without making a fuss'
and
'Client did not take the exercise seriously'
Feedback from those that tried PAM at the Connections peer support group suggested that a minority (36%) were neutral about the effect of Personal Asset Mapping and the majority (64%) thought it was positive. Nobody thought it was negative. One person commented
'It was interesting although it didn't really do anything for me.'
Others said they would not continue to use or develop their Personal Asset Map because
'I can picture these in my mind' and 'at the moment too much in my mind at the present time finding it difficult to concentrate'
(this person said they might look at it again in future) and
'I can't be bothered.'
Practitioners thought that asset mapping might have negative effects if someone is very ill at the time they first try it. The majority (6/9) of the practitioners' diaries specifically mentioned taking care to offer a Personal Asset Mapping session only to people who were judged not to be too ill. They said their choice of which people in their caseload to try it with was based, e.g. on whether the person they would be able to 'work towards a goal' at the time. Those practitioners whose caseload includes people subject to compulsory measures said they chose people who were not subject to compulsory measures.
Getting started
Practitioners documented lots of different ways to introduce the opportunity to create a Personal Asset Map. There were no patterns in what was most successful. Practitioners introduced it with reference to their own map, to the community map as a new thing, in order to help others, for its likely benefits and just as something to try. Seven out of 30 (33%) people who were offered the chance to try PAM one-to-one declined. These people were put off by either:
- The nature of the tool, which they perceived to be 'childish'. For example a practitioner reported
'Person was 18 years old, I think he felt threatened or insulted initially that the tool appeared child like. He stated that he was an adult'
or - It being a new approach (i.e. not wanting to be a guinea pig or not wanting to try new things at all)
A smaller proportion of those who were offered the opportunity to try it in the Connections Peer-Support Group (11%) declined, however this could simply be explained by members not wishing to be the 'odd one out' whilst everyone else in the group was doing Personal Asset Mapping.
Practitioners were initially cautious about who they should introduce it to and started out with various strategies. After trying it they realised it was hard to predict who it might benefit, for example
'I was taken aback, what I initially thought (about which people would be receptive to trying it) was virtually opposite. I felt as if I had really achieved something. I had broken down some barriers; discussions about matters never talked about were brought to the forefront.'
Practitioners concluded that PAM should be offered to everyone as long as they were not in a particularly bad state of mind on the day.
Barriers to widespread use of Personal Asset Mapping in the public sector
Time and role
Even for the enthusiastic practitioner, making time for asset mapping may be an ongoing barrier; the mean time spent supporting someone to create their first asset map was reported as 78 minutes, with 120 minutes the maximum and 25 minutes the minimum time spent. Some practitioners reported time constraints on the length of appointment and what has to be achieved in appointments. Finding time to do PAM was very hard for those involved in statutory interventions
'Given the timescales and nature of the work I do (often crisis based interventions) I would not have much scope to do things differently'
. Whilst it is possible that, with practice, the average time needed to create a first map might decrease, if these structural aspects are not addressed by an explicit change in role and accompanying performance management then it is unlikely that Personal Asset Mapping would be widely adopted. For example practitioners commented
'If I was doing more long-term work then there may be more scope to apply the tool'
and
'There's a disconnect between the values base (that asset mapping is founded on) and the way the local authority can work these days. The voluntary sector is in a much stronger position to pursue this sort of therapeutic tool.'
Towards the end of the project practitioners were invited to continue offering asset mapping and to ask for feedback on these experiences. They were then asked to feedback on whether they were continuing. Third sector practitioners and the Community Mental Health Peer Support Worker are continuing, but others in the Public Sector do not appear to be yet.
Lack of awareness of limitations of existing practice
Gap between intent and actions
Only a minority (3/14) of practitioners initially reported that they thought they could be doing more to help people identify factors that promote their well-being (in the baseline survey). There was therefore a mismatch between the high degree of importance they placed on helping people identify assets, their low level of knowledge of available assets, and low interest in doing more. Another indicator that there is a gap between what practitioners perceived and actual practice is the response from attendees at the peer support group, 36% of whom said that practitioners hadn't done enough to help them identify their assets in the past. Even with the support of the project, one practitioner in particular did not appear to learn to focus on assets during the project; in their reflective diary they talked largely about how they work with people to identify their problems despite having purported to have an assets -focused approach.
Need for more adaptive, facilitative practice in the statutory sector
At the start of the project, practitioners' ideas about how they could encourage people to use assets were limited to making people aware of assets, the benefits of assets and how assets may be used. In some cases, raised awareness of an asset may be sufficient to encourage someone to draw on it or use it more. However many commentators have postulated that awareness is a necessary but insufficient condition for behaviour change (See for example, Swann et al, 2009). To increase use of assets it is necessary for practitioners facilitate a conversation that redirects the person's attention to the assets available, some of the comments made by practitioners indicate that there was a degree of uncertainty about how to achieve this and therefore further support would be required. For example one reported
'One person (I was supporting) seemed unsure what to do once the map was created- how to use it'
when in fact the point was that they needed to be in a position to help the individual think about what to do with it.
The conclusion that some practitioners lack confidence to adapt their way of working and facilitate solutions is reinforced by the difficulty that some health sector and council practitioners had in being asked to develop and test the approach rather than being presenting the finished approach with instructions. The third sector practitioners appeared less affected by this. For the statutory sector then, a gap in adaptive skills (see e.g. Heifetz and Laurie, 1997) affects not just this project but any approach to development of new practice with the frontline.
Barriers to use of PAM to potential
Some types of assets were not mapped
In contrast to the proof of concept project in 2011 (where the categories of 'people', 'places' and 'activities' were used), practitioners were given a blank canvas and were asked to develop their own prompts to encourage people to think about different types of assets.
However, when asked, most practitioners responded using variants of the original categories and as a consequence assets mapped are not as broad as the sorts of assets that are known to promote well-being, e.g. according to Becker (2008) or Antonovsky (1996). Only two practitioners asked this in a slightly different way, e.g. asking people what they spent their time doing and whether they had any hobbies. One practitioner asked about
'supports'
and another about
'protective factors'
In particular personal strengths and skills were not identified, faith did not feature, and the things like nutrition and the home environment tended to be missing. There are gaps in the sorts of assets that attention was drawn to.
Practitioners view on assets did not develop
Before the first workshop, practitioners were asked 'what factors promote well-being?' This question elicited a diverse range of responses suggesting that practitioners had not all been taught or learnt the same thing about what creates health, i.e. knowledge of salutogenic factors is not formalised. Furthermore, nearly half (6/14) practitioners only, or largely, mentioned services as promoting well-being, rather than community resources and things people could do for themselves.
Use of PAM and the Project appeared to have a limited effect on practitioners' knowledge of asset-based theories. In their reflective diaries practitioners were asked to report on the factors they noticed as being that important to the well-being of people they support. Answers given were disappointingly limited. The practitioners who were interviewed were also asked to elaborate on whether their views about what promotes well-being had changed as a result of the project and none of them reported any change.
Learning from community asset mapping
How to generate knowledge of assets
The primary purpose of community asset mapping was to generate a map that could be used in future. This objective was pursued through running workshops and drop-ins at which people were introduced to the idea behind asset mapping and asked to contribute their knowledge of things that promote well-being.
It was harder to attract members of the community to workshops than had been hoped. The workshops were very widely promoted through databases held by EDVA, Long Term Conditions Alliance, East Dunbartonshire CHP, East Dunbartonshire Council and others through the use of 1400 flyers and through the use of 36 posters (placed e.g. in Libraries). Those who did come enjoyed themselves and became more aware of assets. However not many people came (between one and seven members of the public per session), prompting additional workshops e.g. at a skate park with the support of EDVA, at a Dementia Group and at Caring Over Peoples Emotions (COPE) Scotland, a group for carers of people with mental health problems. The drop-ins had a higher attendance because they were located in places with high footfall and they did not require any time commitment from participants. Drop-ins were held during the week and at weekends but with no discernable difference in footfall. The assets contributed at the workshops generally have more qualitative statements associated with them; why people like and use an asset e.g.
'the canal at the S bend looking across the field, its really tranquil and you see lots of wildlife',
whereas drop-ins did generate a significant quantity of assets. 76 assets were contributed via a text-line.
Although attendance at the workshops wasn't high and the people who did attend tended to be 'Community Connectors', i.e. those who held a lot of knowledge about their area, people that were there really enjoyed them. Positive feedback included a good feature of the workshop was
'Interesting about local knowledge and surrounding areas and listening to the input of the younger generation'
or
'Finding out about community facilities in Bishopbriggs that I didn't know about and meeting people'
and
'Learning a lot of new places in Lennoxtown'
The considerable efforts of the CHP and Council to engage people to develop content for this map this mirror learning from many community development projects- it is important to go to where the people are.
On being asked 'what could have been improved?' further praise for the workshop was solicited e.g.
'The workshop was very well done and brilliantly explained- nothing needs changed.'
However some workshop participants thought that more community members should be present and some thought that the map could be bigger.
The workshop format should therefore be maintained and could be run by voluntary organisations and community groups to promote awareness and use of map and stimulate thinking and action on well-being.
Access to and use of the map
Format
Some (mostly) older people were not keen on accessing the Community Well-being Map through a website. Therefore it is necessary to consider how to reach this group.
Framing
At several points throughout the project people made the comment that it was important not to ignore needs. For example participants at the COPE community asset mapping workshop could not proceed until they had aired their views of current services. It is important that, where the public sector is talking about and promoting the Community Well-being Map, it is contextualised as offering wider choice, not replacing services.
Language
Professionals and individuals involved in the personal and community asset mapping found the word 'asset' confusing and suggested a range of different ways to explain it e.g. 'I said to three older men it's a wee exercise to see what things you rely on'. The term well-being was generally more positively received so assets may need to be described as 'things' or perhaps 'resources that promote well-being'.
Costs, activities and financial benefits
Inputs
The project was supported by £18,500 from the Better Together fund and £18,500 from partnership development monies agreed by EDC and East Dunbartonshire CHP. The partners additionally put in staff time in-kind, which amounted to around £60,000 from the CHP. As can be seen from the description of activities below, project staff and partner organisations demonstrated considerable commitment to the project.
Activities
The project started in May 2012 with a launch event attended by around 45 people at which community asset mapping and individual asset mapping were introduced.
Personal Asset Mapping
Support for development of Personal Asset Mapping practice included two Personal Asset Mapping workshops in May and July a reflective session and phone support for a group of 17 mental health practitioners working in the NHS, the Local Authority and the voluntary sector. Practitioners originally agreed to try Personal Asset Mapping with three people that they support and to give feedback about their experiences. Three practitioners who initially signed up did not finish the project for reasons of illness or pressure of work. Not all practitioners who initially signed up tried asset mapping, and not everyone who tried it managed to do so with three people. The PAM approach was also tested with a group of 18 people attending a peer support group. A digital personal asset-mapping tool has been developed as an iPad app, which is to be available for use by practitioners who have been allocated an iPad to work with people they support on developing Personal Asset Maps as appropriate.
Community asset mapping
There were 18 planned community asset mapping workshops and drop-ins held in each town in East Dunbartonshire between June and December 2012. Additional targeted workshops were held with the support of EDVA, COPE and a Dementia carers group. The workshops and drop-ins reached 532 members of the public. A digital community asset map was developed, documenting the assets that had been contributed during the workshops, drop-ins and via a text-line. This was launched as a website at the end of the project.
Project governance
A steering group met most months, and an advisory group met less frequently. Communications included a regularly updated blog. Project staff also represented the project at six 'community gala events' and four Health and Well-being Board events as well as promotion of the project at others' events
Benefits
This project was progressed with the intention to improve quality of service, rather than to save money. As budgets get tighter, attention is inevitably focused on what may save money. There are also some commentators that make theoretical links to the demand on public sector resources that is related to people's capacity to deal with their own problems and to thrive. For example see Evans and Stodart, quoted in Burns (2011). Nonetheless Antonovsky (1996) warns:
The cost-saving claim has hardly been well-documented. (...) My hunch is that one had best make the arguments for health promotion in value rather than in market oriented terms. No one contends that museums pay off in cash.
Focus on assets makes a difference to well-being and this difference may, if pursued at a sufficient scale and over a sufficient length of time achieve a reduction in demand for services, but it is worthwhile in and of itself.
Conclusion and recommendations
Personal Asset Mapping
Personal Asset Mapping is a promising practice that makes a difference to people who use services and improves the extent to which professional practice lives up to intentions to be person-centred recovery focused. Its use should therefore be spread. This project demonstrates that having the visible support of senior management is insufficient to overcome the barriers of time and a sense that it is not the priority focus.Therefore, in order to roll out the practice it will be necessary to support the development of underpinning facilitative skills, to raise awareness across whole teams, and to embed the drivers for its use in e.g. performance management.The forthcoming adoption of the Scottish Recovery Indicator (SRI 2) in East Dunbartonshire may also be supportive of increased attention and sense of support for PAM.
Whilst it is a sensible precaution to consider the state of mind of individuals when considering the timing of introducing them to PAM for the first time, in light of the indications that PAM has either a positive or neutral effect, care should be taken not to restrict the opportunity to try PAM unnecessarily.
Some people perceived the paper version tested in the project to be 'childish'; this appeared to relate to the perception being presented with a box of things like wooden blocks, little figures, stickers, and felt tip pens to make a 3D map with.The iPad app version may be more appealing to some people but equally will put others off, so people should be offered a choice.
The following model (figure 4) has been developed to explain the theory developed in this project from observing and reflecting on accounts of the practice of Personal Asset Mapping. It shows how individuals may be affected by PAM, the expected relationship to well-being, the practitioner input that may be most helpful, and the links to the Community Well-being Map. The model should be referred to and updated as further evidence is generated.
| Theory of change for individual | Effect on Mental Wellbelng | Practitioner Input | Link to CWM |
|---|---|---|---|
| Making initial PAM makes people more aware of what they have (and don't have). | Results from Connections peer group suggest small improvement in mental well-being just from trying PAM. | Practitioner can influence the breadth of what is mapped and how the individual feels about it, e.g. providing reassurance in the event of disappointment. | |
| Discussing and/or reflecting on PAM leads to desire to make improvements. | Not known-potentially negative unless supported to make realistic goals. | Practitioner can influence whether map is used and how it is used. Practitioner supports realistic goals. | Practitioner links to knowledge of community assets |
| Increased self-efficacy in relation to desired changes (not be necessary in all cases) | Increased self-efficacy in and of itself might be positive in terms of mental well-being in the short term. | Practitioner can help people to believe that they can achieve their goals and help them to plan how. | |
| Changes made (e.g. try new asset, make better use of existing asset, change relationships) | Results from one-to-one support suggest large improvement in mental well-being for those people who started to make a change. | Practitioner can support with Practitioner can overcoming any barriers and obstacles. | Practitioner can encourage adding to community well-being map where appropriate. |
| Increased self-efficacy (i.e. made one change so can make others). Revisit map and make new goals. | Possibly long term sustained increase in mental well-being. | Practitioner can remind individual about the map, reinforce success and influence the breadth of goals to focus on a range of salutogenic factors. |
Community Well-being Map
The project has generated a lot of knowledge of community assets and pulled this together in to the useful resource of an on-line Community Well-being Map but this is just the start. Although the website is easy to navigate and use it is unlikely that people will change their behaviour simply as a result of its existence. Therefore the CHP and EDC should support third sector organisations and also well connected community members to run further workshops using the successful format developed by the project in order to ensure a focus on the quality and meaning of the assets is maintained. The CHP and EDC should also raise awareness amongst professionals of the community map and the theory behind promoting assets. Since there are a great number of potential different organisations and routes, these must be prioritised in a communication plan. This must also consider how to reach people who don't use the Internet (e.g. through hard copies in Libraries and/or intergenerational projects)
There are other initiatives to map different categories of assets (e.g. ALISS for people with long term conditions and EDC service directory) the links between these initiatives were explored during the project and EDC and the CHP should continue to work with others to share information on assets and promote complementary initiatives.
For the map to be engaging and used to potential requires continued capture of the meaning of assets and effect of their use.Achieving this will require prompt moderation of comments and that the website is promoted creatively e.g. using polls and surveys to encourage comment and using other social media to connect to it. Therefore the arrangements that are made for the further development and upkeep of the map are crucial to ensuring its continued dynamic development.
The CHP and EDC should now build on the project by considering how to make a system change in attention to, analysis of and use of assets. For example of the range of ways in which an assets culture can be embedded systemically see North West Asset Based Working Steering Group (Undated)
References
- Andresen R, Caputi P, and Oades L (2006). Stages of recovery instrument: development of a measure of recovery from serious mental illness. Australian and New Zealand Journal of Psychiatry, 40(11-12), 972-980.
- Antonovsky A (1979) Health, stress, and coping. San Francisco: Jossey-Bass.
- Antonovsky A (1996) The salutogenic model as a theory to guide health promotion. Health promotion international, 11(1), 11-18.
- Aitken M, Cairns B and Thake S (2008) Community ownership and management of assets, Joseph Rowntree Foundation. Available from: http://www.jrf.org.uk/publications/community-ownership-and-management-assets[Accessed February 2013]
- Beauliue L (2002) Mapping the assets of your community, Southern Rural Development Centre: Mississippi State MS. Available from: http://srdc.msstate.edu/trainings/educurricula/asset_mapping/asset_mapping.pdf[Accessed March 2013]
- Becker, C. et al., 2008. Development and Preliminary Evaluation of a Positive Health Scale. American Journal of Health Education, 39(1), pp.34-41. Available at: http://www.eric.ed.gov/ERICWebPortal/detail?accno=EJ795597 [Accessed January 2013].
- Bogenschneider K and Olson J (Eds) (1998) Building resiliency and reducing risk: What youth need from families and communities to succeed. Available from: http://familyimpactseminars.org/doc.asp?d=s_wifis10exec.pdf [Accessed January 2013]
- Burns H (2011) Health in Scotland in 2010- Assets for Health: Annual report of the Chief Medical Officer, Scottish Government. Available from: http://www.scotland.gov.uk/Resource/0038/00387520.pdf [Accessed March 2013]
- Cook B and Khotari U (2001) Participation: The new tyranny, London: Zed Books
- Czuchry M, Newbern-McFarland D and Dansereau DF(2009) Visual Representation Tools for Improving Addiction Treatment Outcomes. Journal of Psychoactive Drugs, 41(2), p181
- Deacon L et al (2009) North West Mental Well-being Survey, North West Public Health Observatory. Available at: http://www.nwph.net/nwpho/publications/NorthWestMental%20SurveySummary.pdf[Accessed January 2013].
- Emery M and Flora C (2006) Spiraling-up: Mapping community transformation with community capitals framework, Journal of the Community Development Society, Vol. 37 (1)
- Friedli L (2011) Always look on the bright side: the rise of assets based approaches in Scotland, the Poverty Alliance, Scottish Anti-Poverty Review, issue 14. Available at: http://povertyalliance.org/userfiles/files/SAPR_14_Winter1112_FINAL.pdf [Accessed March 2013]
- Graybeal C (2001) Strengths-based social work assessment: Transforming the dominant paradigm, Families in Society: The Journal of Contemporary Human Services, 82, 233-242
- Griffiths T. et al(2007) Life mapping: a 'Therapeutic Document' approach to needs assessment. Quality of Life Research,16(3). p467
- Heifetz, R. A., & Laurie, D. L. (1997). The work of leadership. Harvard business review, 75, 124-134
- Kretzmann JP and McKnight JL (1993) Building communities from the inside out: A path toward finding and mobilizing a community's assets, Evanston, IL: Kretzmann and McKnight
- Lynch H (2008) Lifelong learning, policy and desire, British Journal of Sociology of Education 29 (6), 677-689
- Lynch H and Allan J (2007) Target practice? Using the Arts for Social Inclusion International Journal of Arts and Education 8 (12)1-12
- NHS Confederation (2011) Public mental health and well-being - the local perspective
- North West Asset Based Working Steering Group (Undated). Living well across local communities; prioritising wellbeing to reduce inequalities. Figure 1. Available at: http://www.nmhdu.org.uk/silo/files/the-asset-approach-to-living-well.pdf
- Pattoni L (2012a) strengths-basedapproaches for working with individuals, IRISS.
- Pattoni L (2012b) using an assets approach for positive mental health and well-being, IRISS.
- Roy MJ, Donaldson C, Baker R and Kay A (2012) Social Enterprise: New Pathways to Health and Well-being? Journal of Public Health Policy
- Seligman MEP, Steen TA, Park N, Peterson C (2005) Positive Psychology Progress: Empirical Validation of Interventions. American Psychologist, Vol 60(5), 410-421
- Sigerson and Gruer (2011) Asset-based approaches to health improvement, NHS Health Scotland.
- Stewart-Brown S et al (2009) Internal construct validity of the Warwick-Edinburgh Mental Well-being Scale (WEMWBS): a Rasch analysis using data from the Scottish Health Education Population Survey. Health and Quality of Life Outcomes, 7, p.15. Available at :http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2669062/ [Accessed February 22, 2013].
- Swann et al (2009) Health systems and health-related behaviour change: a review of primary and secondary evidence. Available from: http://www.nice.org.uk/media/0E6/62/SpecialReportHealthSystemsAndHealthRelatedBehaviourChange.pdf [Accessed February 2013]
- Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Weich S, and Stewart-Brown S (2007) The Warwick-Edinburgh mental well-being scale (WEMWBS): development and UK validation. Health and Quality of Life Outcomes, 5(1), p26, p63.
Appendix A Evaluation methodology and discussion
VIE worked with IRISS and other project partners to shape a bespoke approach to evaluation of this project. The evaluation objectives were to:
- During the project to help partners to identify what is working well and what needs to be improved
- To identify and report on the outcomes of the project
The evaluation is effectively a service evaluation for the purposes of service development (See classifications in National Patient Safety Agency 2010) and was therefore judged by the steering committee not to require Ethics Approval. Informed consent was of course sought from individuals participating.
There are a number of commentaries on the need to improve the evidence base of assets approaches. Sigerson and Gruer (2011) assert that important features of evaluation of asset-based approaches include:
- A clear logic model setting out the perceived links between inputs (assets, resources etc.) and outcomes, and the theoretical mechanisms whereby the intervention will result in beneficial change.
- Agreed definitions and measures of the processes and outcomes of the intervention, whether aimed at individuals, groups, communities or larger populations.
- A robust evaluation design including sufficient numbers of participating individuals or communities and sufficient duration of the intervention to be able to confirm or exclude a useful effect; before and after measurements or comparisons with control groups; and measurement of costs.
- An analysis of stakeholder perspectives, particularly of participants, other local community members and relevant service providers.
The intention of this evaluation was to follow these points as closely as possible and thus each point is discussed below.
Logic models
Logic models that document how it was expected that the project would create change were developed and updated throughout the project as the understanding of the results of the project improved. These were initially used as the basis for choice of outcome measure.
Agreed measures
The Warwick Edinburgh Mental Well-being Scale (WEMWBS) was chosen as the primary way to measure outcome on the basis that it measures mental well-being and the primary intended effect of asset mapping is improved well-being. The advantages of WEMWBS are that it is a validated survey instrument, is in use in Scotland as part of the national performance framework and it is designed for individuals to fill in without support and is quick to complete. The possibility of using other approaches to gaining some measure of before and after states was considered, however there is no outcome measurement tool in use in the statutory sector and the implementation of such a tool would be project in itself.
Stewart-Brown and colleagues (2009) propose that surveys like WEMWBS should be subject to a more robust interpretation of the internal construct validity, which is an assessment of whether it is measuring what it is supposed to be measuring (mental well-being). SWEMWBS was found to adhere to a stricter test of internal construct validity than the original WEMWBS. SWEMWBS was used with a group of 18 people trying PAM in a peer support group.
Given the early nature of the work the focus was on generating knowledge about how change happens and can be measured rather than on measurement per-se. Therefore the evaluation process was built around the evaluator accompanying the project by attending as many events and meetings as possible, and co-developing questions and feedback forms that could be used by project staff at events and interactions not attended by the evaluator. The results of feedback were fed back to the project leaders through the steering group and also to the practitioners through a purpose designed reflection session. Reflection on, and response to, these updates was encouraged and a set of reflection prompts was also developed for use by the project leaders.
Evaluation design (in the sense of sample sizes)
The recommendation made at point three of Sigerson and Gruer's recommendations, concerning evaluation design, point to a perceived need to design evaluation in order to determine cause and effect for the end user group. Ignoring for the moment that there is some critique of whether experimental designs are ethical and appropriate for social interactions (rather than drug trials), its full application would effectively push the evaluation into research requiring ethics approval. Early on in the project the project steering group decided that it was impossible, within the limited resources of the project, to establish an experimental design, which requires a randomised assignment of people to two groups that receive or do not receive the intervention. Quasi-experimental approaches were considered and the approach chosen to establishing correlation rested on a pre-intervention and post-intervention well-being survey (the Warwick-Edinburgh Mental Well-being Scale, WEMWBS) to be run with the anticipated group of 54 people who use services trying individual asset mapping for the first time.
Experiences were reported from 21 one-to-one cases, although it is thought that PAM was tried with more individuals. A further 18 individuals were supported to try PAM in a group setting and reports were collected from most of these people.
However, in the end, it was only possible to collect before and after WEMWBS surveys from 16 people who were supported to try Personal Asset Mapping by a mental health practitioner in the usual course of support and a further set of short WEMWBS surveys (SWEMWBS) from a further 13 people who tried Personal Asset Mapping in a group setting. This sample size is unfortunately insufficient to draw strong conclusions.
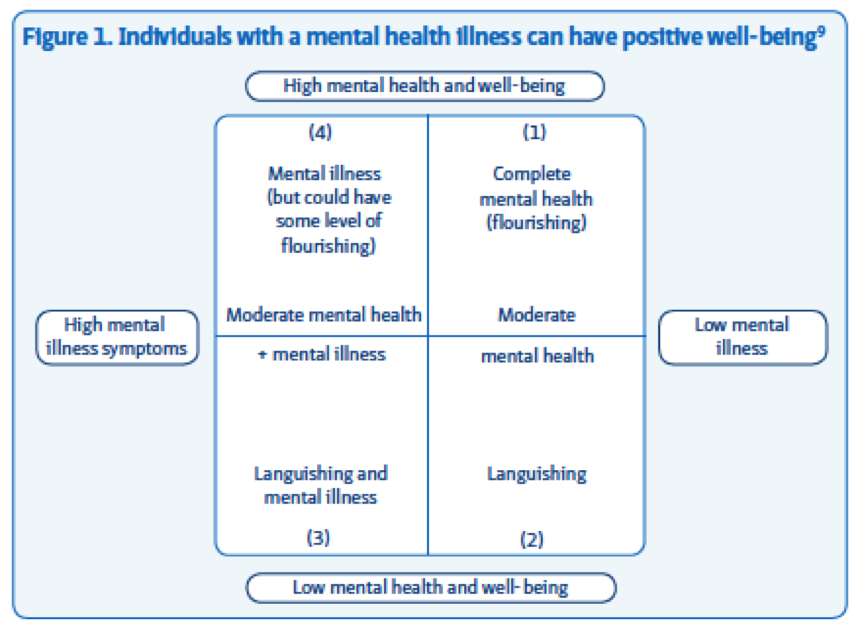
It is also important to note that the concepts of mental well-being and mental health are related but not identical. Others including the NHS Confederation (2011) have commented that it is possible to have some degree of mental well-being even in the case of poor mental health, see figure 5 below. In future therefore it would be worthwhile to track assessments of mental health against assessments of mental well-being.
Analysis of stakeholder perspectives
The emphasis of this evaluation was on gathering and analysing stakeholder perspectives in order to generate deeper knowledge practice and indications of the nature of the impact that approaches might have.
A range of methods was employed to gather these stakeholder perspectives these included:
- A workshop to gather views from people who use services and practitioners who participated in the proof of concept project in 2011.Attendance of the project evaluator at the launch event and direct observation.
- Attendance of the project evaluator at three community asset mapping workshops and direct observation/ interview of participants.
- Design of feedback forms and exercises to be used in other community asset mapping workshops.
- Input to the community asset mapping workshop process including suggestions around questions to ask about the effect of assets, documentation of assets and prioritisation of assets.
- Development of a web-based survey to community asset mapping workshop participants to gather views of the website when it went live.
- Development of a survey of practitioners prior to the first workshop to baseline their experience and attitudes around strengths-based practice
* see figure 6 below for summary of practitioner involvement. - Attendance at the second practitioner workshop and a reflection session. Design of questions and direct observation/ running sessions to gather feedback.
- Semi-structured telephone interview of some practitioners (see figure 6 below).
- Attendance at the two workshops held at the Connections peer support group, design of feedback forms and a reflection session in pairs. Direct observation and interview of participants.
- Semi-structured interview of some people who use services.
- Attendance at most of the steering meetings and feedback to the steering group about evaluation practice.
- Development of reflection questions for project leaders.
| Total | Of which public sector | Of which third sector | |
|---|---|---|---|
| No of practitioners signed up to participate | 17 | 11 | 6 |
| No of practitioners completing baseline survey prior to workshop one | 14 | 10 | 4 |
| No of practitioners completing reflective diary during/after trying Personal Asset Mapping | 9 | 5 | 4 |
| Number of practitioners Interviewed by telephone after trying PAM | 5 | 4 | 1 |