
Key points
- Given the prevalence, severity and impact of fetal alcohol spectrum disorders (FASDs) on individuals and communities, there should be better social work knowledge and understanding of, as well as support for, these disorders
- Social workers can play a more positive role in the prevention and identification of FASD, as well as in services supporting those affected by it
- Increased awareness and learning opportunities, and more encouragement and resources are necessary for social workers to fulfil their potential in this field
Introduction
A fetal alcohol spectrum disorder is an irreversible neurodevelopmental condition caused by alcohol exposure in utero (Mukherjee and Alton (Eds), 2021). FASDs are a significant risk in some, but not all, alcohol-exposed pregnancies. Although not widely known, FASD is the most common learning disability. The Scottish Government estimated that at least 172,000 children, young people and adults currently have FASD (Health Improvement Scotland, 2019).
Anecdotally, we know that social workers rate their knowledge and understanding of FASD as low and would not ordinarily know how to upskill themselves. This Insight is one step toward addressing that gap by covering the long-term impacts of FASD and how social work involvement can support better outcomes for people. Social work support can be preventative, and thereby, reduce escalation, avoid longer-term problems, and help break cycles of vulnerability, marginalisation and adversity.
In an ideal world, social workers would, in the name of social justice, be at the forefront of primary prevention. Unfortunately, that ideal world is not necessarily, or usually the one where most social workers live and work. Frequently, social workers enter the picture ‘after the fact’; that is, once harm has already occurred. Then, the priority is to intervene quickly and decisively to help those affected and to ameliorate the adverse circumstances.
Of course, such a starting point is not unique to social workers. People do not call for an ambulance before a serious illness or injury; just as they do not turn to firefighters before there is a fire to fight.
Why are FASDs relevant to social workers?
While FASD is generally viewed as a medical condition, and within the auspices of the health profession rather than social work, it is a medical condition for which there are no medical solutions.
Social workers may mistakenly view a FASD as a condition that only affects babies and young children, and not people across the lifespan. The term ‘fetal’ can be misleading as no one with this neurodevelopmental condition can ‘outgrow’ it.
The most common manifestations of FASD are cognitive and behavioural, which places them within the remit of social work, education and justice, as well as health.
And while fetal alcohol spectrum disorders have a single direct cause — alcohol-exposure in the womb — there are multiple, indirect causes for drinking alcohol during pregnancy. This underscores the complexity of people’s lives and the value of understanding them in context, of responding to people as individuals and in a holistic and compassionate way.
It is worth remembering that:
- Even if unaware of, or ill-informed about FASD, social workers regularly deal with people who experience this lifelong, life-altering condition (and their families/communities).
- Decisions, plans and actions based on an incomplete or inaccurate knowledge of the complex and multiple roots of troubling behaviours (including FASD) are unlikely to be successful.
- This basic overview will assist social workers in improving how they see, interpret and respond to individuals/families for whom FASD is, or potentially is, a reality.
- It should trigger the reaction that a previously-labelled ‘willful’, ‘bad’ or ‘out of control’ person may actually be neurodiverse, ie, someone unable to behave in a socially-acceptable manner — struggling because of this inability to ‘fit in’.
Given the disproportionate representation among people who are ‘troubled and in trouble’ at home, school and in the care and justice systems, it would be unusual for social workers not to have encountered someone with FASD (Popova and colleagues, 2019). FASD is not rare as it is often perceived to be. And yet, people affected by FASD may not appear on social work’s radar, since fewer than one per cent have been officially diagnosed.
How FASD presents
The effect of FASD on pregnancy was first considered in the 1970s, with a particular focus on the typical facial features shown by some children. Less emphasis was placed on the ongoing, invisible, developmental damage that was being done to the brain.
Alcohol is a teratogen. Like radiation, German Measles and certain medications, such as thalidomide or valproate, alcohol can cause birth defects. Depending on the timing, amount and duration of alcohol exposure, the neurodevelopmental and physiological effects vary considerably. This is because different parts of the fetal body and brain develop at different rates throughout pregnancy. When there are elevated and prolonged levels of alcohol exposure at the earliest stage in gestation, the fetus can develop significant physical problems. These can include the face and palate, heart, eyes, and ears.
Fifty years of extensive international research proved that those with the typical facial features (now referred to as FASD with sentinel facial features) are only the ‘tip of the iceberg’ and represent no more than 10% of all the people living with the adverse consequences of alcohol-exposure during pregnancy (National FASD, 2022).
It was discovered that 90% of children, young people and adults with this neurodevelopmental condition have no facial abnormalities. However, 100% of those affected experience brain and central nervous system consequences. The term ‘fetal alcohol spectrum disorders (FASD) with or without facial features’ is now used worldwide as the more inclusive term.
Health Improvement Scotland published the first comprehensive, evidence-based guidelines in the UK (SIGN 156, 2019) to aid relevant professionals/practitioners make this diagnosis confidently and competently. The guidelines suggest the best ways to support those with a FASD diagnosis and their families. SIGN 156 emphasises the need for multiagency working to achieve optimal outcomes, including social workers (but not as diagnosticians). However, social workers and other agencies working with children and families can help determine the underlying causes of a child’s neurodiversity and if there was prenatal exposure to alcohol.
Potential brain (central nervous system) areas of function for assessment are shown in Figure 1. Assessment occurs across all ten areas in the diagram. Significant deficits in at least three confirm the diagnosis. Individual profiles along this spectrum can be very different.

An illustrative profile of someone with FASD
In practical terms, what would the indicators be for a social worker when considering whether FASD is part of a young person’s life story? Although individual indicators vary greatly, this is an illustrative example of what life might be like for someone with an FASD profile:
I might appear to be very articulate but have problems understanding what you had just told me, as well as keeping track of what I was asked to do to correct my behaviour.
I might be dreadful at keeping appointments and generally organising my life, including poor money concepts and an inability to either plan or follow through on other’s plans for me.
I might be very impulsive without thinking of the consequences; and, even if corrected, I may do it again because I have great difficulty learning from experience.
I might appear truculent and challenging and act inappropriately for my age.
I might be anxious and developing mental health issues because I am being bullied or misunderstood so often.
I might have real skills and talents I am unable to demonstrate consistently because my life is so disorganised and stressful.
I might drink alcohol, take drugs, and engage in other risky behaviours (including sexual ones) because I have a very hard time controlling my impulses.
My sleep pattern will have been poor from an early age.
(Hayes, Moritz and Reid, 2020)

For social workers who wish to get an overview of FASD in less than two hours, the Scottish Government commissioned eLearning resource can be found via NHS Education Scotland's Turas platform. This provides a good starting point.
What social workers need to consider
Social workers will not routinely be expected to ‘diagnose’ FASD, but their knowledge of the child’s functioning, and whether there is a possibility of prenatal alcohol exposure can be crucial in making the diagnosis. Understanding the basics of FASD and what diagnosticians will assess can be helpful when considering a referral.
There continues to be a large gap between the number of people likely to be affected by FASD and those officially diagnosed (Wozniak and Riley, 2019). Still, social workers have opportunities to act helpfully, even in the absence of this diagnosis.
There are three fundamental considerations to be taken into account.
1. Knowledge
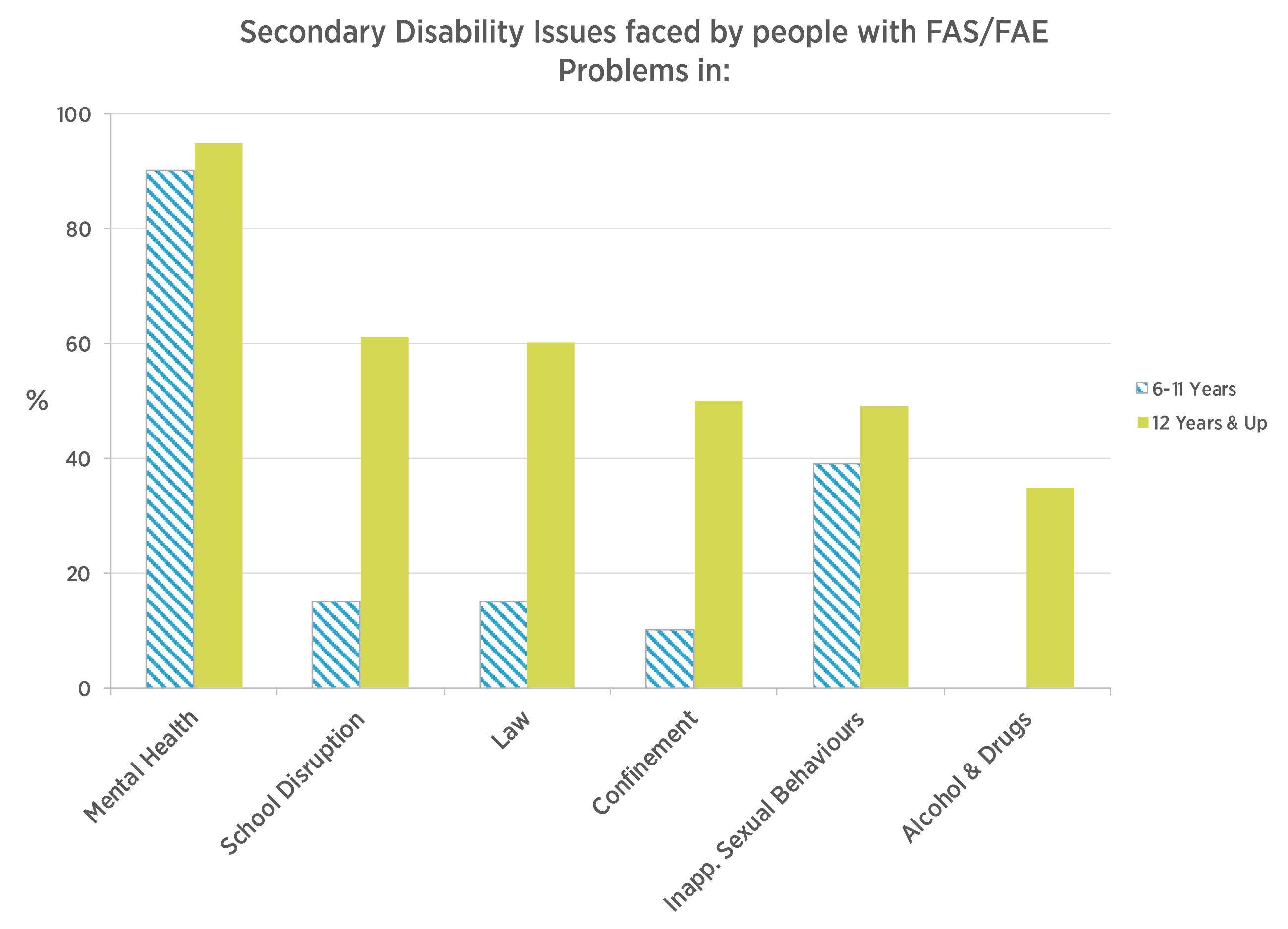
Accurate knowledge about FASD can short-circuit incorrect assumptions and wrong conclusions about people who are troubled, rather than intentional, willful troublemakers. People whose neurodiversity has been overlooked or misunderstood are often prone to ‘secondary’ adversity/disabilities.
For example, school exclusion and petty criminality are not inevitable for people with FASD. However, they become more likely consequences when their neurodiversity is not acknowledged or acted on in practice.
Depression, anxiety disorders, self-harm, and suicidal ideation and action are disproportionately common among individuals whose FASD has contributed to marginalising them.
2. Understanding
Better understanding of FASD can help social workers value their own potential contributions. For example, when a young person engages in unsuccessful serial shoplifting, health professionals are unlikely to become involved. However, an FASD-informed social worker can avert endless repetitions of this story by working with all involved — shopkeeper, family, and police — to help them see the underlying disability, not just the overt behaviour.
Similarly, seeing a Children’s Hearing through a FASD lens could result in placement and support decisions that are likely to have better outcomes because they have considered undiagnosed FASD as a contributing factor requiring further exploration.
Presently, the research literature focuses primarily on the difficulties and deficits experienced by people with FASD. Yet, these same individuals can, and often do, have strengths and positive attributes that should be recognised and built on through social work practice (Skorka and colleagues, 2020).
3. Multiple conditions
Exploring whether complex neurodevelopmental factors are linked to behaviours triggering concern should be explored by social workers. The assessment process should not come to an end as soon as one diagnosable condition is found.
An impressive body of international evidence exists that highlights the frequency of co-existing conditions (Gillberg, 2021). For example, the outdated belief that someone has either ADHD or FASD, but cannot have both simultaneously, has been disproved. The latest scientific research confirms that a person is much more likely to have more than one neurodevelopmental condition, rather than only one (Popova and colleagues, 2016).
Wider implications and tensions in social work practice
Professional identity and role
Professional social workers make up less than 10% of the social care workforce in Scotland. Their distinctive role, according to the International Federation of Social Workers (IFSW, 2014), as well as the more known competencies, also includes ‘the promotion of social change and development.’
The emphasis on ‘social work’ in this Insight is intentional, and purposely avoids the use of the term ‘social care’ which encompasses the combined, wide-ranging disciplines that assist people. It affirms the role of social work where the focus is on enabling and empowering individuals, families, and communities, and protecting human rights and pursuing social justice.
Social work in Scotland has its roots in a model of ‘community social work’, based on social welfare and reflected in the Social Work (Scotland) Act 1968. However, over the decades, a neoliberal agenda has increasingly overtaken that broader social work ethos, emphasising statutory interventions following reported concerns (Turbett, 2018).
The Scottish Government’s flagship Getting It Right for Every Child (GIRFEC, 2016) strategy, while admirable in its intentions, is heavily focused on risk assessment tools. The practical impact — prioritising ‘child rescue’ over ‘family support’ has become a significant issue for social work practitioners (Clapton, 2018). The ‘child’s needs are paramount’ (The Children (Scotland) Act 1995 sec 11 (7) (a) is the associated principle which underpins all assessment and intervention, however, that child must be considered in the context of the family (Stone, 1995, p ix).
This has direct implications for social work practice in relation to FASD. In Scotland, the subject of children affected by parental substance misuse and/or ‘not good enough’ parenting is situated predominantly within child protection practice. Thus, the focus of social work is on the unborn child and any risk factors to which the child may be exposed (Scottish Government, 2021). This work with possibly ‘involuntary clients’ must begin with the recognition that the interaction between worker and the adult client is frequently based on conflict rather than cooperation. Social work with involuntary clients is a political, not a therapeutic process, involving the socially sanctioned use of power (Barber, 1991, p45).
The Promise is informing us on how relationships matter with ‘care experienced young people’. Independent advocacy which supports best social work practice, such as PAR (parents advocacy and rights) services, can assist in informing on and supporting parents’ perspectives.
Relationships and power
In 2018, Dr Ariana Critchley stated: ‘Pre-birth involvement forms a small but increasing part of child protection work in Scotland’ with desirability for ‘good working relationships with parents while protecting the unborn baby from current risk’ (Critchley, 2018). Sadly, numerous factors get in the way of forming these desired good working relationships. The power imbalance between parents and social workers can make relationships of mutual trust and respect difficult to achieve. This is despite best intentions and positive attempts by practitioners to balance perceived need and risk of harm. Short-term measures often consist of investigative and legal processes aimed at protecting the child, which may involve removal from the parents’ care. While this (multi-agency) decision may sometimes appear best for all concerned, better outcomes are not inevitable.
Third sector partners increasingly provide in-depth support which can enable change, and build up a significant knowledge base on early years support. We also know that parents fear being judged and that time is required to build trust, with issues of non-engagement and non-compliance explored in the literature (2022). Some mothers might have underlying issues linked to alcohol misuse and/or mental health challenges, which could be identified and sensitively supported by colleagues in adult social work practice. However, children and family workers need to have the time and opportunity to reflect and consult with others. This is difficult when social workers’ working conditions have worsened over the years, making preventative and relationship-based work increasingly difficult (Ravalier and colleagues, 2021).
Delivering positive outcomes
The State as ‘corporate parent’ does not have an unblemished track record of success. Scotland has the highest number of children being ‘looked after and accommodated’ in the UK, and this has only increased in the past year. (Scottish Government, 2021). More is being learned about the longer-term outcomes of children having been removed from their birth families. FASD, whether recognised or below the radar — and whether a reality for the parent and/or the child — is often ‘in the mix’ of child protection decisions and actions.
Foster and adoptive parents of children with undiagnosed FASD may be faced with difficult and complex behaviours, sometimes escalating to a complete breakdown of the placement. This behaviour may have been erroneously attributed solely to environmental factors, leading to an inaccurate or incomplete diagnosis of, for example, disordered attachment or PTSD. Misdirected ‘therapy’ and delays in seeing and helping with FASD are unlikely to have positive, long-term outcomes.
In kinship care, often young people and adults return to the circles of their birth families or seek knowledge about where they ‘belong’ (Farmer, 2013). This presents a thorny dilemma for social work in Scotland, which merits deeper analysis. Parents’ voices play an increasingly prominent role (PAR, 2021).
Further action
In addition to the points made and resources already identified, here are two recommendations for further action:
- Take FASD prevention seriously through two-sided messaging and meaningful follow-up.
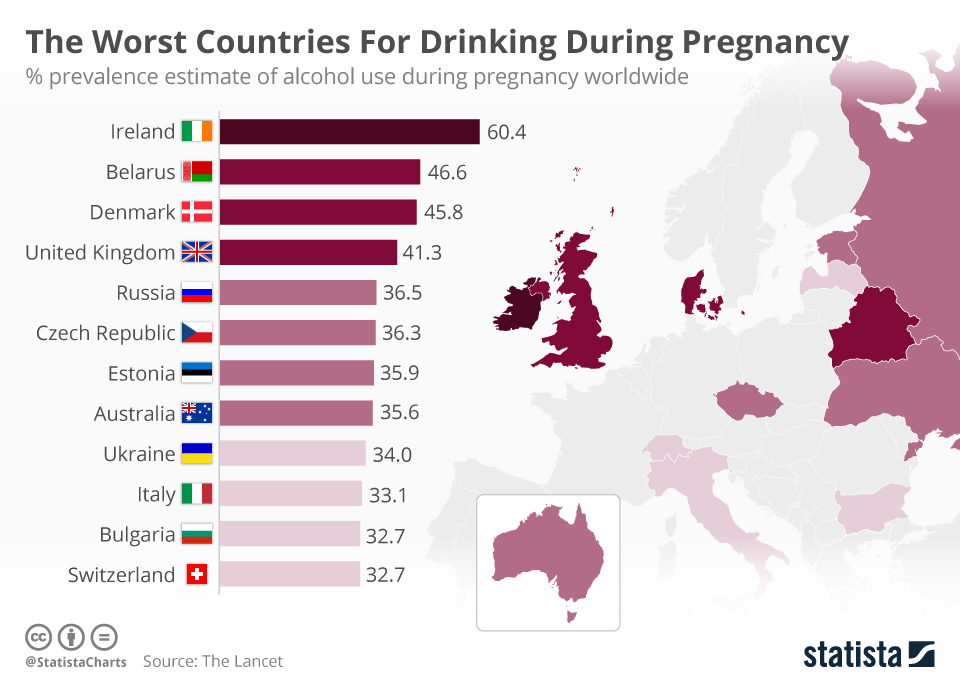
It is commonplace for women in Scotland, and throughout the UK, to drink during pregnancy (Figure 4). Often this is unintentional. We know that at least 40% of pregnancies are unplanned, and therefore, the opportunity to protect the growing fetus is not always possible. This applies to all age groups and social class of women (Abernethy and colleagues, 2018).
And yet, it is very rare for any woman who drinks alcohol during pregnancy to intend to harm her baby. That is why blaming and stigmatising women is cruel, as well as ineffective. On the contrary, respect for good intentions allows social workers to interact positively with women of reproductive age and their partners. In turn, this enables candid, accurate, non-judgmental conversations about alcohol, pregnancy, and the risk of FASD (Plant, 2022).
There are two guaranteed ways to prevent FASD. The first is to consume no alcohol throughout pregnancy. The second is to avoid becoming pregnant while continuing to drink alcohol. No alcohol or no pregnancy. If implemented fully, then both are completely successful strategies for avoiding FASD.
- Continue to learn more about FASD and share that knowledge widely.
Social workers have opportunities to show leadership in helping Scotland succeed in understanding what to know and do about FASD. As examples, this leadership could be applied at social work networks, multiagency meetings, Children’s Hearings or one-to-one contact with clients.
Other OECD countries are further ahead of Scotland and the rest of the UK. The Australian Government recently invested $27 million in a nationwide, multi-year FASD prevention initiative, as well as equal investment in FASD services, support and research. International research, policies, practices and support provide a foundation of cumulative wisdom and experience on which Scotland can build.
The Scottish Government currently provides support for FASD-related professional development through the following two organisations.
The FASD Hub — the first of its kind in the UK — was launched in 2019 to provide help primarily to the parents/carers of children and young people known, (or believed) to have been affected, by alcohol exposure during pregnancy. It operates an active national helpline, Facebook peer support groups, and workshops and training for families and health and social care professionals.
The Fetal Alcohol Advisory and Support Team (FAAST) is a Scottish Government funded programme at the University of Edinburgh. The emphasis is on improving professional knowledge and confidence in working with people affected by FASD. It also promotes service development, mainly across Scotland’s Health and Social Care Partnerships, while maintaining a best practice and research evidence base.
Final thoughts
When referrals are made because of concerns about a child’s wellbeing and/or a woman’s drinking, social workers with an understanding of FASD can argue persuasively to give priority to engaging constructively and compassionately with mothers/parents. The goal is to develop relationships of mutual trust and respect that lead to better outcomes for all concerned. This needs time, effort, interpersonal skills and basic FASD knowledge. Such work is what social workers enjoy and are good at (Bryan and colleagues, 2016).
Having a more than superficial understanding of FASD and how to support those affected should make an important difference in the trajectory of that person’s and family’s life. People with FASD are often perceived as ‘being the problem,’ as opposed to being recognised as ‘having a disability’ (Loock and colleagues, 2020).
Key to best social work practice is multi-disciplinary collaboration, which should not only involve health, justice, and education professionals, but also the third sector, parental advocacy organisations and, crucially, women/parents and families. Developments such as Family Group Decision Making are helpful innovations enabling positive outcomes (Corwin and colleagues, 2021).
FASD is both present and harmful. The authors of this Insight believe that social work has a vital role to play in preventing this neurodevelopmental condition and that it is social work’s role to campaign for social justice by tackling underlying reasons for alcohol use. When prevention of FASD has not been possible, social work also has a vital role to play in helping and supporting Scotland’s individuals, families and communities to achieve their best possible lives.
References
- Abernethy C, McCall KE, Cooper G et al (2018) Determining the pattern and prevalence of alcohol consumption in pregnancy by measuring biomarkers in meconium. Archives of Disease in Child Fetal and Neonatal Edition 2018, 103, F216–F220
- Alcohol Focus Scotland (2018) Parental drinking in Scotland 2018
- Barber JG (1991) Beyond casework. Basingstoke: MacMillan Education
- Begun AL (2020) Social environmental contexts of addictive behavior. In Begun LA and Murray MM (eds) The Routledge handbook of social work and addictive behaviours. New York: Routledge, 110-128
- Bryan A, Hingley-Jones H and Ruch G (2016) Relationship based practice revisited. Journal of Social Work Practice, 30, 2016
- Bronfenbrenner U (1979) The ecology of human development. Harvard University Press
- Choi S and Ryan JP (2007) Co-occurring problems for substance abusing mothers in child welfare: matching services to improve family reunification. Children and Youth Services Review, 29, 11, 1395−1410
- Clapton G (2018) Social work with children and families. In Cree V and Smith M Social work in a changing Scotland. Oxfordshire: Routledge, 11, 111-121
- Critchley A (2018) Pre-birth child protection, Iriss Insight 42. Glasgow: Iriss
- Corwin TW, Maher EJ, Merkel-Holgui L et al (2020) Increasing social support for child welfare-involved families through family group conferencing. The British Journal of Social Work, 50, 1, 137-156
- Curry L (2022) Scotland’s care system for children and young people. Edinburgh: The Scottish Parliament
- Education Scotland (2021) Nurture, adverse childhood experiences and trauma informed practice: making the links between these approaches. Livingston: Education Scotland
- Farmer E (2013) The reunification of looked after children with their parents: what contributes to return stability? The British Journal of Social Work, 43, 8, 1611–1629
- Farmer E (2022) Reunification from out-of-home care: a research overview of good practice in returning children home from care. Bristol: University of Bristol
- Ferguson H (2020) From snapshots of practice to a movie - researching long-term social work and child protection by getting as close as possible to practice and organisational life. British Journal of Social Work, 2020, 50, 1706-1723
- Ferguson H, Warwick L, Disney T et al (2022) Relationship-based practice and the creation of therapeutic change in long-term work: social work as a holding relationship. Social Work Education, The International Journal, 41, 2
- Gillberg C (2021) The ESSENCE of autism and other neurodevelopmental conditions: rethinking c-morbidities, assessment and intervention. London: Jessica Kingsley
- Gilbert D, Mukherjee R, Kassam N et al (2021) Exploring the experiences of social workers in working with children suspected to have fetal alcohol spectrum disorders. Adoption and Fostering, 45, 2, 155-172
- Hayes N, Moritz KM and Reid N (2020) Parent-reported sleep problems in school-aged children with fetal alcohol spectrum disorder: association with child behaviour, caregiver, and family functioning. Sleep Medicine, 74, 307-314
- Hillen P (2018) Social work and substance misuse. In Cree V and Smith M, Social work in a changing Scotland. Oxfordshire: Routledge, 17, 171-180
- Hines AM, Lee PA, Osterling KL et al (2007) Factors predicting family reunification for African American, Latino, Asian and White families in the child welfare system. Journal of Child and Family Studies, 16, 275–89
- Holmes L and McDermid S (2012) Understanding costs and outcomes in child welfare services. London: Jessica Kingsley
- International Federation of Social Workers (2014) IFSW: Global definition of social work
- Loock C, Elliot E and Vitale Cox L (2020) Fetal alcohol spectrum disorder, evidence, theory, and current insights. In Begun L and Murray M, The Routledge handbook of social work and addictive behaviours. Oxfordshire: Routledge
- McGruer F and Shields J (2018) FAAST study mental health - key findings
- Mukherjee R and Alton N (2021) Prevention, recognition and management of fetal alcohol spectrum disorders. New York: Springer
- National Institute for Health and Care Excellence (2022). Fetal alcohol spectrum disorder: quality standard. London: NICE
- National Organisation for FASD (2022)The time is now.
- PAR (2021) Parents advocacy and rights
- Plant M (2022) Women, alcohol, pregnancy and FASD. The Queen’s Nursing Institute Scotland
- Popova S, Lange S, Shield K et al (2016) Comorbidity of fetal alcohol spectrum disorder: a systematic review and meta-analysis. The Lancet.
- Popova S, Lange S, Shield K et al (2019) Prevalence of fetal alcohol spectrum disorder among special subpopulations: a systematic review and meta-analysis, Addiction, 114, 7, 1150-1172.
- Ravalier JM, McFadden P, Boichat C et al (2021) Social worker wellbeing: a large mixed methods study. The British Journal of Social Work, 51, 1, 297–317
- Scottish Government (1995) Children (Scotland) Act 1995 section 11 (7) (a) Children (Scotland) Act 1995
- Scottish Government (2007) Adult support and protection (Scotland) Act 2007 Adult Support and Protection (Scotland) Act 2007
- Scottish Government (2011) Children’s Hearing (Scotland) Act 2011 sec 67 2 (n) Children's Hearings (Scotland) Act 2011
- Scottish Government (2014) Chapter 3: Principles and definition of adult at risk - adult support and protection revised code of practice
- Scottish Government, (2016) GIRFEC National Practice Model
- Scottish Government (2021) Children looked after - children's social work statistics: 2019 to 2020
- Scottish Government (2021) National guidance for child protection in Scotland
- Scottish Intercollegiate Guideline Network (2019) (SIGN) 156: Children and young people exposed prenatally to alcohol
- Skorka K, McBryde C, Copley J et al (2020) Experiences of children with fetal alcohol spectrum disorder and their families: a critical review. Alcoholism: Clinical and Experimental Research, 44, 6, 1175-1188
- Smith N (2002) Reunifying families affected by maternal substances abuse: consumer and service provider perspectives on the obstacles and the need for change. Journal of Social Work Practice in the Addictions, 2, 33–53
- Smith M, Gallacher M, Wosu H et al (2012) Engaging with involuntary service users in social work: findings from a knowledge exchange project. British Journal of Social Work, 42, 1460–1477
- Stone FH (2003) Report of the expert committee on how to deal with children in trouble which influenced the establishment of the Children’s Hearing system. In The Kilbrandon report. Edinburgh: Scottish Government
- Streissguth AP, Bookstein FL, Barr HM et al (2004) Risk factors for adverse life outcomes in fetal alcohol syndrome and fetal alcohol effects. Dev Behav. Ped. 25, 4, 228-38
- The Promise Scotland (2021) Whole family support
- Togher N (2022) Understanding disguised non-compliance in social work. Glasgow: Iriss
- Turbett C (2018) Community social work in Scotland: a critical history. Glasgow: Iriss
- Wilkins D and Forrester D (2021) What do parents think about statutory child and family social work services in the UK? The British Journal of Social Work, 51, 2210-2227
- Wozniak J R and Riley EP (2019) Clinical presentation, diagnosis, and management of fetal alcohol spectrum disorder. The Lancet Neurology, 18, 8, 760-770
Resources
Scotland
- Alcohol Focus Scotland
- FASD Scotland
- FASD Hub Scotland
- FAAST Team
- Oshay’s
- Scottish Government Neurodevelopmental Pathway
- Scottish Alcohol Research Network (SARN)
- Scottish Health Action on Alcohol Problems (SHAAP)
- Queen’s Nursing Institute Scotland
UK
International
Acknowledgements
- From the FAAST Team, University of Edinburgh:
- Dr Suzanne O’Rourke
Senior Lecturer in Forensic Clinical Psychology, University of Edinburgh
Consultant in Forensic, Clinical and Neuropsychology, State Hospitals Board for Scotland - Dr Jennifer Shields
Consultant Clinical Psychologist, CAMHS NHS Western Isles
Lecturer in FASD, University of Edinburgh
- Dr Suzanne O’Rourke
- Dr Helen Albutt (NHS Education Scotland)
- Dr Arianne Critchley (University of Stirling)
- Dr Christopher Steer — B.Sc.(Hons) M.B. Ch.B. (Edin) DCH.(Glasg) FRCPE. FRCPCH. Consultant Paediatrician. Hon Senior Lecturer (Ret), SHAAP Steering Committee member for 10 yrs, representing RCPCH
- Dr Amy Chandler (University of Edinburgh)
- Dr Maggie Watts (Public Health, NHS Western Isles)
- Caroline McDonald (North West Health and Social Care Partnership)
- Scottish Gov colleagues from the Scottish Government Learning Disabilities and Autism Policy Team
- Julie Lusk (Professional Social Work Adviser for Adult Mental Health, Directorate of Mental Health, Scottish Government)
About the authors
Trisha Hall became a social worker in the UK after a career in further education in the Netherlands. She worked in the statutory as well as the third sector, and was the National Director of The Scottish Association of Social Work (part of BASW UK) for over six years until retirement from full time work in 2019. Trisha now has some part time involvement as Associate Tutor at the Faculty of Social Sciences at the University of Stirling. She also supports the Cattanach Trust through Board membership and is involved in some local voluntary work.
Dr Patricia D. Jackson (OBE, FRCPCH) is a neurodevelopmental paediatrician with many years’ experience of working with children and young people with varying types of neurodiversity in Scotland. She is an Honorary Fellow with the University of Edinburgh, Department of Child Life and Health, and also continues her voluntary role as a trained Children’s Panel member. In 2019 she chaired the Health Improvement Scotland committee that published the National guideline ‘SIGN 156 — Children and Young People exposed prenatally to alcohol.’ She continues to input to resources and teaching courses to improve awareness and understanding of FASD.
Dr Jonathan Sher is a Senior Fellow and Programme Lead for Healthier Pregnancies, Better Lives at the Queen’s Nursing Institute Scotland. Prior to moving to Scotland 17 years ago, he was President (Chief Executive) of the North Carolina Child Advocacy Institute. Jonathan was also a faculty member and Associate Dean in the University of North Carolina system. Starting in 2005, Jonathan was Director of Research, Policy and Programmes at Children in Scotland. His last assignment there (a decade ago) was writing the UK’s first online course about Fetal Alcohol Spectrum Disorders. In 2020, he was one of five co-authors (including Dr Patricia Jackson) of the SG/NHS Education for Scotland FASD eLearning resource. Jonathan was a Children’s Parliament Trustee.
Credits
- Series Coordinator: Kerry Musselbrook
- Commissioning Editor: Kerry Musselbrook
- Copy Editor: Michelle Drumm
- Designer: Ian Phillip